105
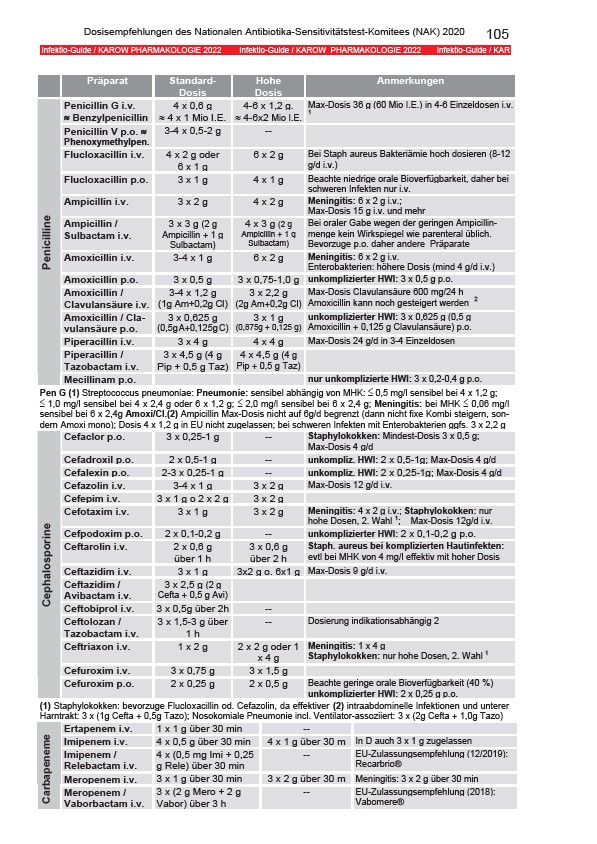
Dosisempfehlungen des Nationalen Antibiotika-Sensitivitätstest-Komitees (NAK) 2020
Infektio-Guide / KAROW PHARMAKOLOGIE 2022 Infektio-Guide / KAROW PHARMAKOLOGIE 2022 Infektio-Guide / KAR
Präparat Standard-
Dosis
Hohe
Dosis
Anmerkungen
Penicillin G i.v.
≈ Benzylpenicillin
4 x 0,6 g
≈ 4 x 1 Mio I.E.
4-6 x 1,2 g.
≈ 4-6x2 Mio I.E.
Max-Dosis 36 g (60 Mio I.E.) in 4-6 Einzeldosen i.v.
1
Penicillin V p.o. ≈
Phenoxymethylpen.
3-4 x 0,5-2 g --
Flucloxacillin i.v. 4 x 2 g oder
6 x 1 g
6 x 2 g Bei Staph aureus Bakteriämie hoch dosieren (8-12
g/d i.v.)
Flucloxacillin p.o. 3 x 1 g 4 x 1 g Beachte niedrige orale Bioverfügbarkeit, daher bei
schweren Infekten nur i.v.
Ampicillin i.v. 3 x 2 g 4 x 2 g Meningitis: 6 x 2 g i.v.;
Max-Dosis 15 g i.v. und mehr
Ampicillin /
Sulbactam i.v.
3 x 3 g (2 g
Ampicillin + 1 g
Sulbactam)
4 x 3 g (2 g
Ampicillin + 1 g
Sulbactam)
Bei oraler Gabe wegen der geringen Ampicillinmenge
kein Wirkspiegel wie parenteral üblich.
Bevorzuge p.o. daher andere Präparate
Amoxicillin i.v. 3-4 x 1 g 6 x 2 g Meningitis: 6 x 2 g i.v.
Enterobakterien: höhere Dosis (mind 4 g/d i.v.)
Amoxicillin p.o. 3 x 0,5 g 3 x 0,75-1,0 g unkomplizierter HWI: 3 x 0,5 g p.o.
Amoxicillin /
3-4 x 1,2 g
3 x 2,2 g
Clavulansäure i.v.
(1g Am+0,2g Cl)
(2g Am+0,2g Cl)
Max-Dosis Clavulansäure 600 mg/24 h
Amoxicillin kann noch gesteigert werden 2
Amoxicillin / Clavulansäure
p.o.
3 x 0,625 g
(0,5g A+0,125g C)
3 x 1 g
(0,875g + 0,125 g)
unkomplizierter HWI: 3 x 0,625 g (0,5 g
Amoxicillin + 0,125 g Clavulansäure) p.o.
Piperacillin i.v. 3 x 4 g 4 x 4 g Max-Dosis 24 g/d in 3-4 Einzeldosen
Piperacillin /
3 x 4,5 g (4 g
4 x 4,5 g (4 g
Tazobactam i.v.
Pip + 0,5 g Taz)
Pip + 0,5 g Taz)
Penicilline
Mecillinam p.o. nur unkomplizierte HWI: 3 x 0,2-0,4 g p.o.
Pen G (1) Streptococcus pneumoniae: Pneumonie: sensibel abhängig von MHK: ≤ 0,5 mg/l sensibel bei 4 x 1,2 g;
≤ 1,0 mg/l sensibel bei 4 x 2,4 g oder 6 x 1,2 g; ≤ 2,0 mg/l sensibel bei 6 x 2,4 g; Meningitis: bei MHK ≤ 0,06 mg/l
sensibel bei 6 x 2,4g Amoxi/Cl.(2) Ampicillin Max-Dosis nicht auf 6g/d begrenzt (dann nicht fixe Kombi steigern, sondern
Amoxi mono); Dosis 4 x 1,2 g in EU nicht zugelassen; bei schweren Infekten mit Enterobakterien ggfs. 3 x 2,2 g
Cefaclor p.o. 3 x 0,25-1 g -- Staphylokokken: Mindest-Dosis 3 x 0,5 g;
Max-Dosis 4 g/d
Cefadroxil p.o. 2 x 0,5-1 g -- unkompliz. HWI: 2 x 0,5-1g; Max-Dosis 4 g/d
Cefalexin p.o. 2-3 x 0,25-1 g -- unkompliz. HWI: 2 x 0,25-1g; Max-Dosis 4 g/d
Cefazolin i.v. 3-4 x 1 g 3 x 2 g Max-Dosis 12 g/d i.v.
Cefepim i.v. 3 x 1 g o 2 x 2 g 3 x 2 g
Cefotaxim i.v. 3 x 1 g 3 x 2 g Meningitis: 4 x 2 g i.v.; Staphylokokken: nur
hohe Dosen, 2. Wahl 1; Max-Dosis 12g/d i.v.
Cefpodoxim p.o. 2 x 0,1-0,2 g -- unkomplizierter HWI: 2 x 0,1-0,2 g p.o.
Ceftarolin i.v. 2 x 0,6 g
über 1 h
3 x 0,6 g
über 2 h
Staph. aureus bei komplizierten Hautinfekten:
evtl bei MHK von 4 mg/l effektiv mit hoher Dosis
Ceftazidim i.v. 3 x 1 g 3x2 g o. 6x1 g Max-Dosis 9 g/d i.v.
Ceftazidim /
3 x 2,5 g (2 g
Avibactam i.v.
Cefta + 0,5 g Avi)
Ceftobiprol i.v. 3 x 0,5g über 2h --
Ceftolozan /
3 x 1,5-3 g über
Tazobactam i.v.
1 h
-- Dosierung indikationsabhängig 2
Ceftriaxon i.v. 1 x 2 g 2 x 2 g oder 1
x 4 g
Meningitis: 1 x 4 g
Staphylokokken: nur hohe Dosen, 2. Wahl 1
Cefuroxim i.v. 3 x 0,75 g 3 x 1,5 g
Cephalosporine
Cefuroxim p.o. 2 x 0,25 g 2 x 0,5 g Beachte geringe orale Bioverfügbarkeit (40 %)
unkomplizierter HWI: 2 x 0,25 g p.o.
(1) Staphylokokken: bevorzuge Flucloxacillin od. Cefazolin, da effektiver (2) intraabdominelle Infektionen und unterer
Harntrakt: 3 x (1g Cefta + 0,5g Tazo); Nosokomiale Pneumonie incl. Ventilator-assoziiert: 3 x (2g Cefta + 1,0g Tazo)
Ertapenem i.v. 1 x 1 g über 30 min --
Imipenem i.v. 4 x 0,5 g über 30 min 4 x 1 g über 30 m In D auch 3 x 1 g zugelassen
Imipenem /
4 x (0,5 mg Imi + 0,25
Relebactam i.v.
g Rele) über 30 min
-- EU-Zulassungsempfehlung (12/2019):
Recarbrio®
Carbapeneme Meropenem /
Meropenem i.v. 3 x 1 g über 30 min 3 x 2 g über 30 m Meningitis: 3 x 2 g über 30 min
Vaborbactam i.v.
3 x (2 g Mero + 2 g
Vabor) über 3 h
-- EU-Zulassungsempfehlung (2018):
Vabomere®