201
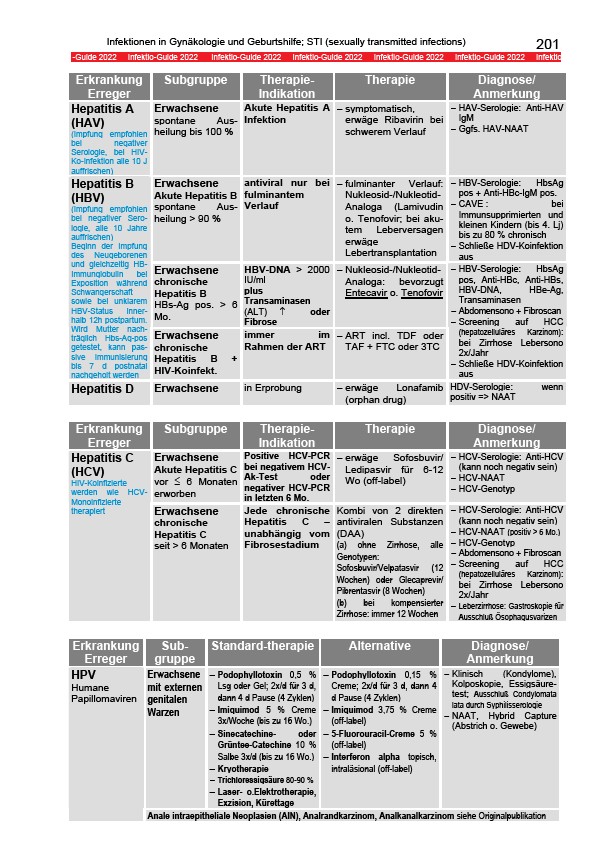
Infektionen in Gynäkologie und Geburtshilfe; STI (sexually transmitted infections)
-Guide 2022 Infektio-Guide 2022 Infektio-Guide 2022 Infektio-Guide 2022 Infektio-Guide 2022 Infektio-Guide 2022 Infektio
Erkrankung
Subgruppe Therapie-
Therapie Diagnose/
Erreger
Indikation
Anmerkung
Hepatitis A
(HAV)
(Impfung empfohlen
bei negativer
Serologie, bei HIVKo
Infektion alle 10 J
auffrischen)
Erwachsene
spontane Ausheilung
bis 100 %
Akute Hepatitis A
Infektion
− symptomatisch,
erwäge Ribavirin bei
schwerem Verlauf
− HAV-Serologie: Anti-HAV
IgM
− Ggfs. HAV-NAAT
Erwachsene
Akute Hepatitis B
spontane Ausheilung
> 90 %
antiviral nur bei
fulminantem
Verlauf
− fulminanter Verlauf:
Nukleosid-/Nukleotid-
Analoga (Lamivudin
o. Tenofovir; bei akutem
Leberversagen
erwäge
Lebertransplantation
− HBV-Serologie: HbsAg
pos + Anti-HBc-IgM pos.
− CAVE : bei
Immunsupprimierten und
kleinen Kindern (bis 4. Lj)
bis zu 80 % chronisch
− Schließe HDV-Koinfektion
aus
Erwachsene
chronische
Hepatitis B
HBs-Ag pos. > 6
Mo.
HBV-DNA > 2000
IU/ml
plus
Transaminasen
(ALT) ↑ oder
Fibrose
− Nukleosid-/Nukleotid-
Analoga: bevorzugt
Entecavir o. Tenofovir
Hepatitis B
(HBV)
(Impfung empfohlen
bei negativer Serologie,
alle 10 Jahre
auffrischen)
Beginn der Impfung
des Neugeborenen
und gleichzeitig HBImmunglobulin
bei
Exposition während
Schwangerschaft
sowie bei unklarem
HBV-Status innerhalb
12h postpartum.
Wird Mutter nachträglich
Hbs-Ag-pos
getestet, kann passive
Immunisierung
bis 7 d postnatal
nachgeholt werden
Erwachsene
chronische
Hepatitis B +
HIV-Koinfekt.
immer im
Rahmen der ART
− ART incl. TDF oder
TAF + FTC oder 3TC
− HBV-Serologie: HbsAg
pos, Anti-HBc, Anti-HBs,
HBV-DNA, HBe-Ag,
Transaminasen
− Abdomensono + Fibroscan
− Screening auf HCC
(hepatozelluläres Karzinom):
bei Zirrhose Lebersono
2x/Jahr
− Schließe HDV-Koinfektion
aus
Hepatitis D Erwachsene in Erprobung − erwäge Lonafamib
(orphan drug)
HDV-Serologie: wenn
positiv => NAAT
Erkrankung
Erreger
Subgruppe Therapie-
Indikation
Therapie Diagnose/
Anmerkung
Erwachsene
Akute Hepatitis C
vor ≤ 6 Monaten
erworben
Positive HCV-PCR
bei negativem HCVAk
Test oder
negativer HCV-PCR
in letzten 6 Mo.
− erwäge Sofosbuvir/
Ledipasvir für 6-12
Wo (off-label)
− HCV-Serologie: Anti-HCV
(kann noch negativ sein)
− HCV-NAAT
− HCV-Genotyp
Hepatitis C
(HCV)
HIV-Koinfizierte
werden wie HCVMonoinfizierte
therapiert Erwachsene
chronische
Hepatitis C
seit > 6 Monaten
Jede chronische
Hepatitis C –
unabhängig vom
Fibrosestadium
Kombi von 2 direkten
antiviralen Substanzen
(DAA)
(a) ohne Zirrhose, alle
Genotypen:
Sofosbuvir/Velpatasvir (12
Wochen) oder Glecaprevir/
Pibrentasvir (8 Wochen)
(b) bei kompensierter
Zirrhose: immer 12 Wochen
− HCV-Serologie: Anti-HCV
(kann noch negativ sein)
− HCV-NAAT (positiv > 6 Mo.)
− HCV-Genotyp
− Abdomensono + Fibroscan
− Screening auf HCC
(hepatozelluläres Karzinom):
bei Zirrhose Lebersono
2x/Jahr
− Leberzirrhose: Gastroskopie für
Ausschluß Ösophagusvarizen
Erkrankung
Erreger
Subgruppe
Standard-therapie Alternative Diagnose/
Anmerkung
Erwachsene
mit externen
genitalen
Warzen
− Podophyllotoxin 0,5 %
Lsg oder Gel; 2x/d für 3 d,
dann 4 d Pause (4 Zyklen)
− Imiquimod 5 % Creme
3x/Woche (bis zu 16 Wo.)
− Sinecatechine- oder
Grüntee-Catechine 10 %
Salbe 3x/d (bis zu 16 Wo.)
− Kryotherapie
− Trichloressigsäure 80-90 %
− Laser- o.Elektrotherapie,
Exzision, Kürettage
− Podophyllotoxin 0,15 %
Creme; 2x/d für 3 d, dann 4
d Pause (4 Zyklen)
− Imiquimod 3,75 % Creme
(off-label)
− 5-Fluorouracil-Creme 5 %
(off-label)
− Interferon alpha topisch,
intraläsional (off-label)
− Klinisch (Kondylome),
Kolposkopie, Essigsäuretest;
Ausschluß Condylomata
lata durch Syphilisserologie
− NAAT, Hybrid Capture
(Abstrich o. Gewebe)
HPV
Humane
Papillomaviren
Anale intraepitheliale Neoplasien (AIN), Analrandkarzinom, Analkanalkarzinom siehe Originalpublikation