Mykosen 280
Infektio-Guide / KAROW PHARMAKOLOGIE 2022 Infektio-Guide / KAROW PHARMAKOLOGIE 2022 Infektio-Guide / KAR
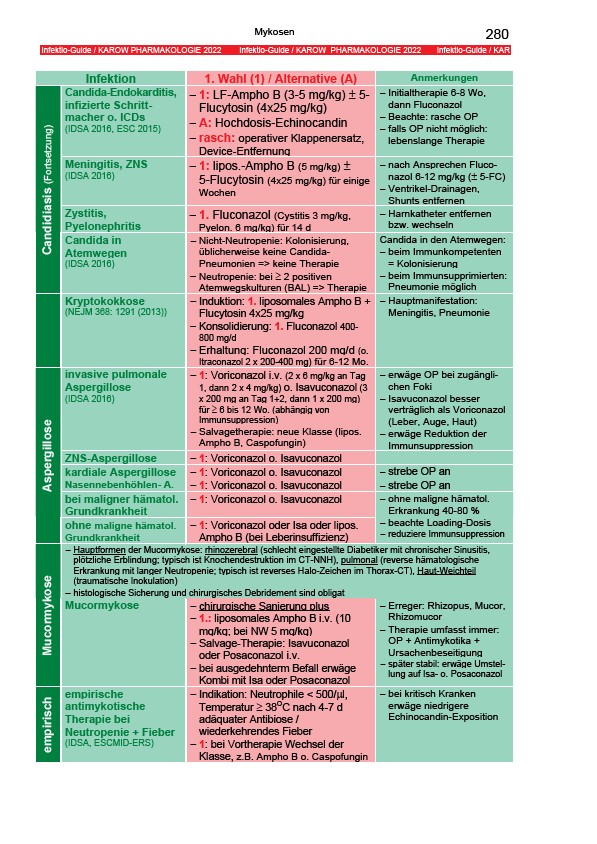
Infektion 1. Wahl (1) / Alternative (A) Anmerkungen
Candida-Endokarditis,
infizierte Schrittmacher
o. ICDs
(IDSA 2016, ESC 2015)
− 1: LF-Ampho B (3-5 mg/kg) ± 5-
Flucytosin (4x25 mg/kg)
− A: Hochdosis-Echinocandin
− rasch: operativer Klappenersatz,
Device-Entfernung
− Initialtherapie 6-8 Wo,
dann Fluconazol
− Beachte: rasche OP
− falls OP nicht möglich:
lebenslange Therapie
Meningitis, ZNS
(IDSA 2016)
− 1: lipos.-Ampho B (5 mg/kg) ±
5-Flucytosin (4x25 mg/kg) für einige
Wochen
− nach Ansprechen Fluconazol
6-12 mg/kg (± 5-FC)
− Ventrikel-Drainagen,
Shunts entfernen
Zystitis,
Pyelonephritis
− 1. Fluconazol (Cystitis 3 mg/kg,
Pyelon. 6 mg/kg) für 14 d
− Harnkatheter entfernen
bzw. wechseln
Candidiasis (Fortsetzung)
Candida in
Atemwegen
(IDSA 2016)
− Nicht-Neutropenie: Kolonisierung,
üblicherweise keine Candida-
Pneumonien => keine Therapie
− Neutropenie: bei ≥ 2 positiven
Atemwegskulturen (BAL) => Therapie
Candida in den Atemwegen:
− beim Immunkompetenten
= Kolonisierung
− beim Immunsupprimierten:
Pneumonie möglich
Kryptokokkose
(NEJM 368: 1291 (2013))
− Induktion: 1. liposomales Ampho B +
Flucytosin 4x25 mg/kg
− Konsolidierung: 1. Fluconazol 400-
800 mg/d
− Erhaltung: Fluconazol 200 mg/d (o.
Itraconazol 2 x 200-400 mg) für 6-12 Mo.
− Hauptmanifestation:
Meningitis, Pneumonie
invasive pulmonale
Aspergillose
(IDSA 2016)
− 1: Voriconazol i.v. (2 x 6 mg/kg an Tag
1, dann 2 x 4 mg/kg) o. Isavuconazol (3
x 200 mg an Tag 1+2, dann 1 x 200 mg)
für ≥ 6 bis 12 Wo. (abhängig von
Immunsuppression)
− Salvagetherapie: neue Klasse (lipos.
Ampho B, Caspofungin)
− erwäge OP bei zugänglichen
Foki
− Isavuconazol besser
verträglich als Voriconazol
(Leber, Auge, Haut)
− erwäge Reduktion der
Immunsuppression
ZNS-Aspergillose − 1: Voriconazol o. Isavuconazol
kardiale Aspergillose − 1: Voriconazol o. Isavuconazol − strebe OP an
Nasennebenhöhlen- A. − 1: Voriconazol o. Isavuconazol − strebe OP an
bei maligner hämatol.
− 1: Voriconazol o. Isavuconazol
Grundkrankheit
Aspergillose
ohne maligne hämatol.
Grundkrankheit
− 1: Voriconazol oder Isa oder lipos.
Ampho B (bei Leberinsuffizienz)
− ohne maligne hämatol.
Erkrankung 40-80 %
− beachte Loading-Dosis
− reduziere Immunsuppression
− Hauptformen der Mucormykose: rhinozerebral (schlecht eingestellte Diabetiker mit chronischer Sinusitis,
plötzliche Erblindung; typisch ist Knochendestruktion im CT-NNH), pulmonal (reverse hämatologische
Erkrankung mit langer Neutropenie; typisch ist reverses Halo-Zeichen im Thorax-CT), Haut-Weichteil
(traumatische Inokulation)
− histologische Sicherung und chirurgisches Debridement sind obligat
Mucormykose
Mucormykose − chirurgische Sanierung plus
− 1.: liposomales Ampho B i.v. (10
mg/kg; bei NW 5 mg/kg)
− Salvage-Therapie: Isavuconazol
oder Posaconazol i.v.
− bei ausgedehnterm Befall erwäge
Kombi mit Isa oder Posaconazol
− Erreger: Rhizopus, Mucor,
Rhizomucor
− Therapie umfasst immer:
OP + Antimykotika +
Ursachenbeseitigung
− später stabil: erwäge Umstellung
auf Isa- o. Posaconazol
empirisch
empirische
antimykotische
Therapie bei
Neutropenie + Fieber
(IDSA, ESCMID-ERS)
− Indikation: Neutrophile < 500/μl,
Temperatur ≥ 38OC nach 4-7 d
adäquater Antibiose /
wiederkehrendes Fieber
− 1: bei Vortherapie Wechsel der
Klasse, z.B. Ampho B o. Caspofungin
− bei kritisch Kranken
erwäge niedrigere
Echinocandin-Exposition